Case Study
Wouter Roosink, Master Physician Assistant (mpa), Department of surgery, Maasstad Hospital Rotterdam, The Netherlands
Introduction
The following case will describe our journey together with miss K.
In April of the year 2019 Miss K. underwent a Hartman procedure because of a complicated diverticulitis. As usual we placed a colon stoma during the Hartman procedure. In the days after surgery we saw a slow recovery. There was some leakage of her abdominal wound so we took out one of her stitches and start flushing her wound.
Miss K. left the hospital in a good condition with medical home care to take care of her abdominal wound.
In the following weeks minor problems start to occur. The abdominal wound is getting bigger , 3 by 5 cm and approximately 2 cm in depth. There are also slight problems fitting the stoma material next to the abdominal wound dressing. This results in regular leakage of her stoma.
In de weeks that follow the wound is getting bigger, 5 by 15 cm, and the skin is undermined with some cavity’s. At this point the wound is treated with aquacell.
There was a small bridge of skin between her stoma and the wound edge which gave problems in wound and stoma care. There was a lot of leakage from the wound and the stoma. Eventually caudal in the wound a hefty abscess spontaneously relieved itself. Large amounts of pus start leaking out of the wound that caused the wound to be barely treatable on our outpatient clinic
Miss K. was admitted to our surgical ward with the request to gain better control in managing this complex case.
Methods
We regularly see problematic abdominal wounds in our surgical department. One of our major challenges is the treatment of entero- cutaneous fistulas. Since over a year we have been using fistula adapters to guide the faeces out of the wound and treat the rest of the wound with V.A.C. VERAFLO™ or plain vacuum therapy.
We saw some very good results of that kind of treatment.
At the surgical ward we were confronted with a wound of 5 by 15 cm with a lot of undermining of the skin. There was a lot of outflow of pus that needed bandage change up to 6 times a day. Despite regular change in bandage there was still a lot of leakage witch gave miss K a lot of discomfort.
There was also a skin bridge of several centimeters between the stoma and the edge of the wound. As a result, it was impossible to apply vacuum therapy.
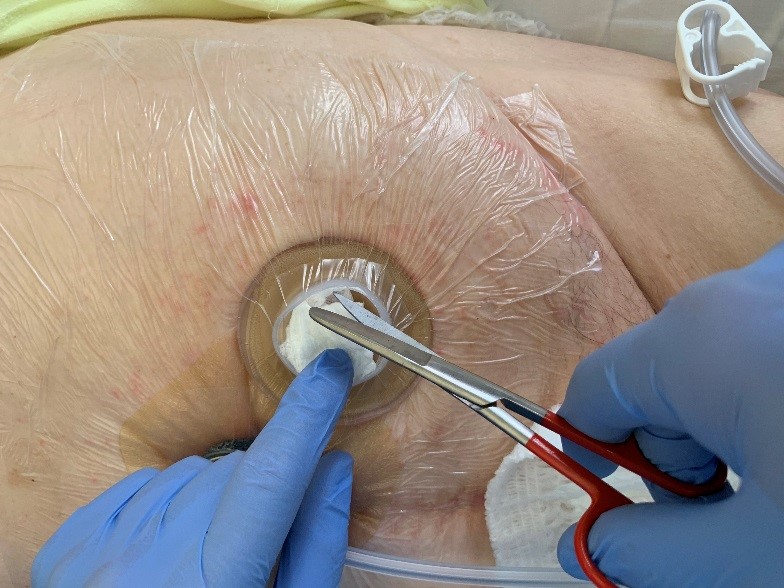
After very intensive conversation with miss K. and her family, we decided to consider the stoma as a kind of entero-cutaneous fistula. With this decision we started to include the stoma inside our zone of vacuum therapy.




*In the picture above you can see an ordinary vac system instead of the V.A.C. VERAFLO™. This photograph was later made when the Vera flow already changed for normal vacuum therapy.

After 3 days we performed a wound inspection. We noticed a significant improvement of the wound. The wound had a calm aspect and showed a good blood flow. There was no longer outflow of pus, even in the subcutaneous cavities there was no pus anymore.
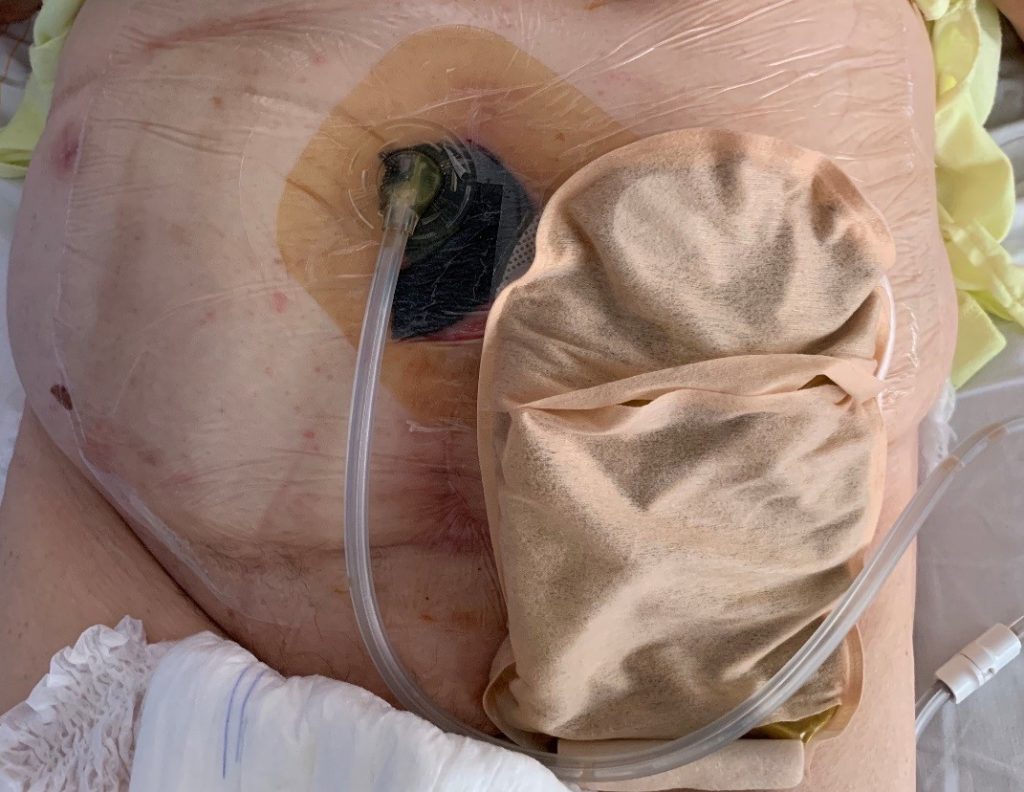
It was decided to change to a normal vacuum system with 100 mmHg. The wound crown® was used as described earlier.
Around the 3rd exchange of the vacuum system miss K. and her family had enough confidence to go home with home care. The vacuum system was changed 2 times a week, once a week at home and once a week at the outpatient clinic.
Before discharge, a specialist team of home care came to see how the vacuum system was installed and learned how to manage problems when they occur.
Results
The system was immediately effective . There was no leakage of the wound and because the stoma material now fits much better in combination with vacuum foil there was no leakage of the stoma anymore.
It was no
longer necessary to give woundcare during the day
As a result, miss K. felt better and regain the confidence to move around
without being afraid of leakage. She came out of bed again. She also slept much
better.
We did not
only see a big improvement of the wound, we also saw a big improvement in her
behavior. Miss K. was now much more active, happier and not as scared as she
was before.
After the second vacuum change there has been a single liquid and air leakage, this could be solved by replacing a part of the sponge and improving the sealing at the Wound crown® .
Unfortunately, after discharge the system proved difficult to handle at home. Also at the outpatient clinic there was trouble keeping the system working properly. In both cases, the lack of knowledge and the fear of a new system proved to be the reason for this problem.
Finally, in consultation with Miss K. we decided to stop the vacuum system. Luckily the wound had become much smaller in the meantime and the stoma material and the bandage material could easily be placed next to each other so that the previous extreme complicated situation was no longer there.
At the moment Miss K. is in analysis to remove her stoma and close the abdominal wound.
Discussion
The applied vacuum system with wound crown® immediately proves itself, giving better control of the wound and the overall situation.
Because it
is a newly applied technique, there is only a small group of people in our
hospital who can manage this way of vacuum therapy. When problems occur in the
evening, night or weekend it’s very dependent on who is on duty that shift.
this results in a lot of time investment from a small group when starting up
this treatment.
It also proves difficult to have this vacuum therapy carried out at home and at the outpatient clinic because of the lack of knowledge and fear of a new system. This creates a quick tendency to leave treatment and to step back to known ways of wound care.
Conclusion
The use of V.A.C. VERAFLO™ in combination with a wound crown® has proven its added value in clinical setting. We saw a fast improvement of the wound, it gives the patient more comfort and the nursing staff spends less time on woundcare. Both Miss K and the nursing staff are excited about this way of wound care. Since this is still a relatively new concept, the expertise currently only exists in a small group of healthcare professionals. As a result, in the hours of service it is sometimes difficult to solve a problem with the vacuum system. It has also been found that there is a large gap between home care ,outpatient clinic and clinic in terms of care for this particular vacuum system. This seems to be mainly explained by lack of knowledge and the fear of a new system. It is therefore necessary for the future to continue training and teach colleagues about this technique. At the moment, the vacuum system in clinical setting is easy to handle and hopefully after good training and information soon usable in home care setting.