Case Study
Introduction. Negative-pressure wound therapy (NPWT) with instillation is a major advancement in the treatment of infected complex wounds. It adds the benefits of topical solution instillation to the known beneficial properties of negative-pressure therapy.
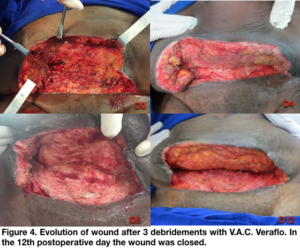
Methods. A 54 year-old female underwent hysterectomy through a transverse abdominal incision (pfannenstiel incision) due to leiomyomatosis by the Gynecology and Obstetrics team of our institution. The patient had diabetes, obesity and hypertension. She had a superficial partial dehiscence and she was discharged at the 6th postoperative day. She returned to the our hospital at the 13th operative day with increase of the wound dehiscence, fever and abdominal pain (Figure 1). The lab work showed signs of systemic infection (leucocytosis and PCR elevation). The Plastic Surgery was called for evaluation and it was indicated surgery in the same day. She had a surgical debridement of the skin and fat in the abdominal flap (Figure 2). The abdominal wall was closed. She underwent V.A.C. Veraflo application (Figure 3). The device pressure was set to 125 mmHg for 4 hours with instillation of normal saline in the intervals (80 ml for 20 minutes). She had new debridements each 4 days with intensive wound lavage and Veraflo changing during 8 days (first Veraflo application plus 2 changes). In the 12th postoperative day (4th Plastic Surgery team procedure) the would was clean and with granulation. So the patient was submitted to a surgical closure with layered abdominal flap closure (Figure 4).
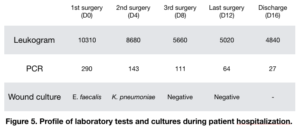
Results. The closure was successful and the patient was discharged at the 16th postoperative day. The cultures at the day of the closure were negatives. The patient had gradual and continuous decreasing of the lab work results after the performed procedures (Figure 5). After 3 weeks of the last surgery the patient was performing daily activities. And after 6 weeks she was able to return to the previous activity level she had before the initial surgery (Figure 6).
Discussion. The properties of traditional NPWT are several such as stimulation of wound granulation, reduction of edema, reduction of excess fluid and wound debris and reduction of bacterial colonization in the wound. The association of NPWT with solution instillation has the potential to increase wound cleaning by debris removal, help in infectious combat by dilution of microorganisms and destruction of the biofilm. It appears that the NPWT with instillation’s greatest appeal, due to its properties, is in the case of complex, contaminated or infected wounds. In these cases, NPWTi has the potential to allow a smaller number of surgical interventions and to reach an earlier definitive wound closure.
Conclusion. The use of negative-pressure wound therapy with instillation was vital for the successful resolution of this severe wound infection with systemic repercussion.