Case Study
Introduction:
In 2010 = 200 million people world wide with Peripheral Arterial disease including Europe ((Lajoie,2019)
Over 170 million people world wide have Diabetes & 366 million by 2030 (Thiruvoipati, T. et al . 2015)
Contributing Factors
- Diabetes(Berg,2018)
- Smoking
- Hypertension
- ↑ Cholesterol
- Age/Male (≥60 y/o)
- Obesity/(Mohler and M, 2017)(Fowkes et al., 2013) \’NPWT creates an environment that promotes wound healing by preparing the wound bed for closure, reduce oedema, promote granulation tissue formation and perfusion and removing exudate and infectious material\’ Fernandez, L (Chronic Wound Care Management & Research) Dovepress
Case Study: Elective Metatarsal Right foot Amputation
A 54- year- old female admitted on the 13.05.2019 for an elective Transmetatarsal right foot amputation. Mrs X is known type 2 diabetic, on daily peritoneal dialysis, pericarditis in the past, and left eye cataract surgery and Vetrictomy and anterior chamber intraocular lens replacement 19.08.19. Prior to this admission, Mrs X is independently mobile, and self caring. Doesn\’t smoke or drink alcohol. She lives alone.
Investigations/Findings:
Triphasic flow CFA, proximal PFA. SFA and PopA diffuse minor disease waveforms gradually becoming pulsatile borderline monophasic due to severe calcification.
Echo:
Mild concentric LVH. normal LV cavity size and systolic function .Mild abnormal septal motion.EF visually estimated at 55%. grade 1 diastolic dysfunction. Mildly dilated LA :normal RV &RA.
Operative Tissue sample showed infection
Diagnosis: Elective admission for Transmetatarsal amputation right foot due to PVD
Co-morbidities:
- Pain { Pain team specialist to control the pain involved}
- Infection { Microbiologist input for the right treatment and duration of intravenous antibiotics}
- Diabetes {Diabetes nurse specialist monitoring for controlled blood sugar }
- Mobility {Vascular Physiotherapist input for mobility function exercises}
- Low mood { Phycologist input and medication for low mood}
- Low appetite {weekly weight monitoring and dietician input for high protein diet and drink supplement}
Initial Treatment of Therapy:
Transmetatarsal right foot amputation 13.05.19 under GA. Post operative wound reviewed 48 hours after. Wound was commenced on alternate days autolytic dry dressing with silver for 2 weeks. Wounds remain non healing and producing thick slough and oozing.
week 3 Mrs X was commenced on NPWT using black foam after MDT discussion with patient verbal consent, on a 125mmHg pressure, continuously on a high intensity. Dressing changed every after 3-4 days for 2 weeks. Wound remains sloughy, thick and very slow healing progress. Had wound debridement in theatre, then commenced on NPWTi-d using VERAFLO CLEANSE CHOISE dressing foam.
Week 5 on VERAFLO 125mmHg: 30 mls normal saline instillation,10 minutes soak time every 3 1/2hours





Mrs X was continuously practising with her transfer with the vascular physiotherapist until safe to go back to her own place.
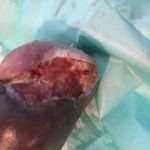
Sept 19, 2019 Mrs X was discharged from hospital to her own place, with district nurse input for wound care (daily inadine dressing).
Wound on discharge date sept. 19, 2019

Discharge and Follow -up:
Podiatry, Mr Mark Portou\’s vascular clinic,opthalmology and diabetes clinic appoitment in 2 weeks time after discharge.
Clinical Outcomes/conclusion;
Mrs X wound management was challenging to us all clinicians or on the multidisciplinary team. Considering that Mrs X is a diabetic patient, with peripheral vascular disease and other co-morbidities, her pain tolerance as well is very low….and using this wound management, was more challenging. It requires patience, planning and strategies. Her compliance and patience was extra ordinary because of her faith to us, clinicians and to the equipment we use VERAFLO using CLEANSE CHOICE dressing. However, there are factors to consider ,in any wound healing, like nutrition, pain control, mobility, infection free, patient cooperation and good blood flow. Good wound assessment, staff knowledge and choice of the right equipment. As evidenced to Mrs X wound management journey using the veraflo cleanse choice, we found that, this kind of therapy we chose was more effective than to ordinary V.A.C. based from the type of wound that Mrs X has.

Reference:
Vascular Surgical Ward
The Royal Free NHS Foundation Trust Hampstead London, NW3 2QG
consultant/Physician
Mr C Lim & Mr Mark Portou